
In 1916, Dr. E.B. Cragin delivered an address entitled "Conservatism in Obstetrics" to the Eastern Medical Society of New York in which he coined the phrase "Once a caesarean, always a caesarean."
For most of the twentieth century, doctors followed this dogma believing that once a woman delivered by C/S she should deliver all future pregnancies by repeat C/S. Clinical studies starting the 1960s, however, concluded that this practice was not always necessary.
In 1980, the National Institutes of Health (NIH) Consensus Development Conference Panel questioned the necessity of routine repeat Cesarean Section. After extensive research, the panel made recommendations regarding the VBAC. Their recommendations gave support to the practice of the TOLAC and successful VBAC with a significant rise in the number of attempted VBAC from the 1980s through 1996.
A major turning point occurred in 1996 with a study published in The New England Journal of Medicine (MacMahon et al, 1996) which concluded that a vaginal delivery after previous C/S (VBAC) was associated with an increased maternal complications as compared to the Elective Repeat Cesarean Section (ERCS).
The American College of Obstetrics and Gynecology (ACOG) subsequently issued guidelines in its 1999 Practice Bulletin which recommended that "VBAC should be attempted in institutions equipped to respond to emergencies with physicians immediately available to provide emergency care." (ACOG, 1999) This practice bulletin also recommended that a physician "capable of monitoring labor and performing an emergency cesarean delivery" be "immediately available throughout active labor," and that anesthesia and personnel for an emergency cesarean be "available."
Logistical and professional liability issues led many hospitals to restrict or prohibit the practice of VBAC. As a result, the rate at which VBAC was attempted fell from 26% in the early 1990s to less than 10% today.
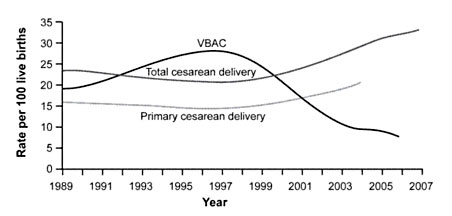
Figure 1. Rates of Total Cesarean Deliveries, Primary Cesarean Deliveries, and Vaginal Birth After Cesarean (VBAC), 1989 to 2007. Data from the National Center for Health Statistics.
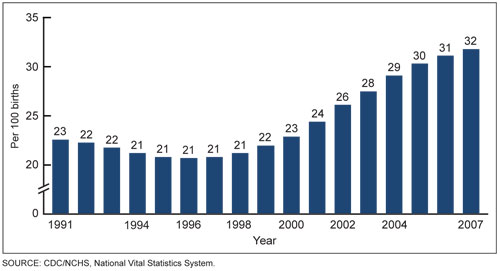
Figure 2. Increasing Rates of Cesarean Section, 1991 to 2007. Data from the US Department of Health and Human Services.
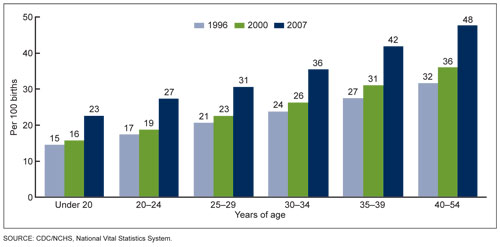
Figure 3. Cesarean delivery rates by age of mother. United States, 1998, 2000 & 2007. Data from the US Department of Health and Human Services.
In March 2010, the National Institutes of Health (NIH) hosted its Consensus Development Conference on the subject of VBAC and concluded, "Given the available evidence, trial of labor is a reasonable option for many pregnant women with one prior low transverse uterine incision.".
Also in March 2010, the U.S. Department of Health and Human Services (HHS), Agency for Healthcare Research and Quality (AHRQ) reported that VBAC is a reasonable and safe choice for the majority of women with a history of prior C/S and that there is emerging evidence of serious harm relating to multiple Cesarean Sections.
In July 2010, The American Congress of Obstetricians and Gynecologists (ACOG) similarly revised their own guidelines to be less restrictive of VBAC, stating, "Attempting a vaginal birth after cesarean (VBAC) is a safe and appropriate choice for most women who have had a prior cesarean delivery, including for some women who have had two previous cesareans."
There is an association between C/S delivery and abnormal placental position and growth in subsequent pregnancies. This risk begins following the first C/S and increases with each subsequent C/S, especially after 4 C/S. Therefore, it is important to consider this risk in women wanting to have large families.
The incidence of placenta previa (placenta covering the cervix) significantly increases in women with each additional C/S delivery:
The presence of placenta previa is also associated with an increased incidence of placenta accreta, increta, and percreta.
Under normal circumstances, the placenta attaches to the uterine wall in the upper portion of the uterus (fundus) and it does so like a suction cup without deeply penetrating into the uterine tissue or muscle. Placenta Accreta, Increta and Percreta are all abnormal and potentially life threatening attachments of the placenta into muscle and sometimes through the entire uterine wall to include adjacent organs such as the bladder and rectum.

Placenta accreta is an invasion of the myometrium which does not penetrate the entire thickness of the uterine muscle. It is the most common form of the condition and accounts for 75-78% of cases.
Placenta increta occurs when the placenta further extends into the myometrium, penetrating deeper into the muscle. This represents 17% of cases.
Placenta percreta represents the worst of this condition, when the placenta penetrates the entire myometrium through the entire uterine wall. This variant can lead to the placenta attaching to other organs such as the rectum or bladder. This represents 5-7% of cases.
If you have a life-threatening emergency, call 911. If your matter is an emergency (only) and you need to speak to Dr. Novoa concerning this emergency after the office has closed, please call 951.595.9944 (Wait for the prompt and you will be connected to Dr. Novoa). If you have a question that is not an immediate emergency, please call during office hours. A nurse or physician will assist you as soon as possible.

10781 Pebble Hills, Suite A
El Paso, TX 79935
915.595.9944
915.996.9074
Monday - Friday:
9:00am - 5:00pm